Accuracy of the Enhanced Liver Fibrosis Test vs FibroTest, Elastography, and Indirect Markers in Detection of Advanced Fibrosis in Patients With Alcoholic Liver Disease.
Gastroenterology
Thiele M, Madsen BS, Hansen JF, Detlefsen S, Antonsen S, Krag A
2018 Gastroenterology Volume 154 Issue 5
PubMed 29317276 DOI 10.1053/j.gastro.2018.01.005
BACKGROUND & AIMS
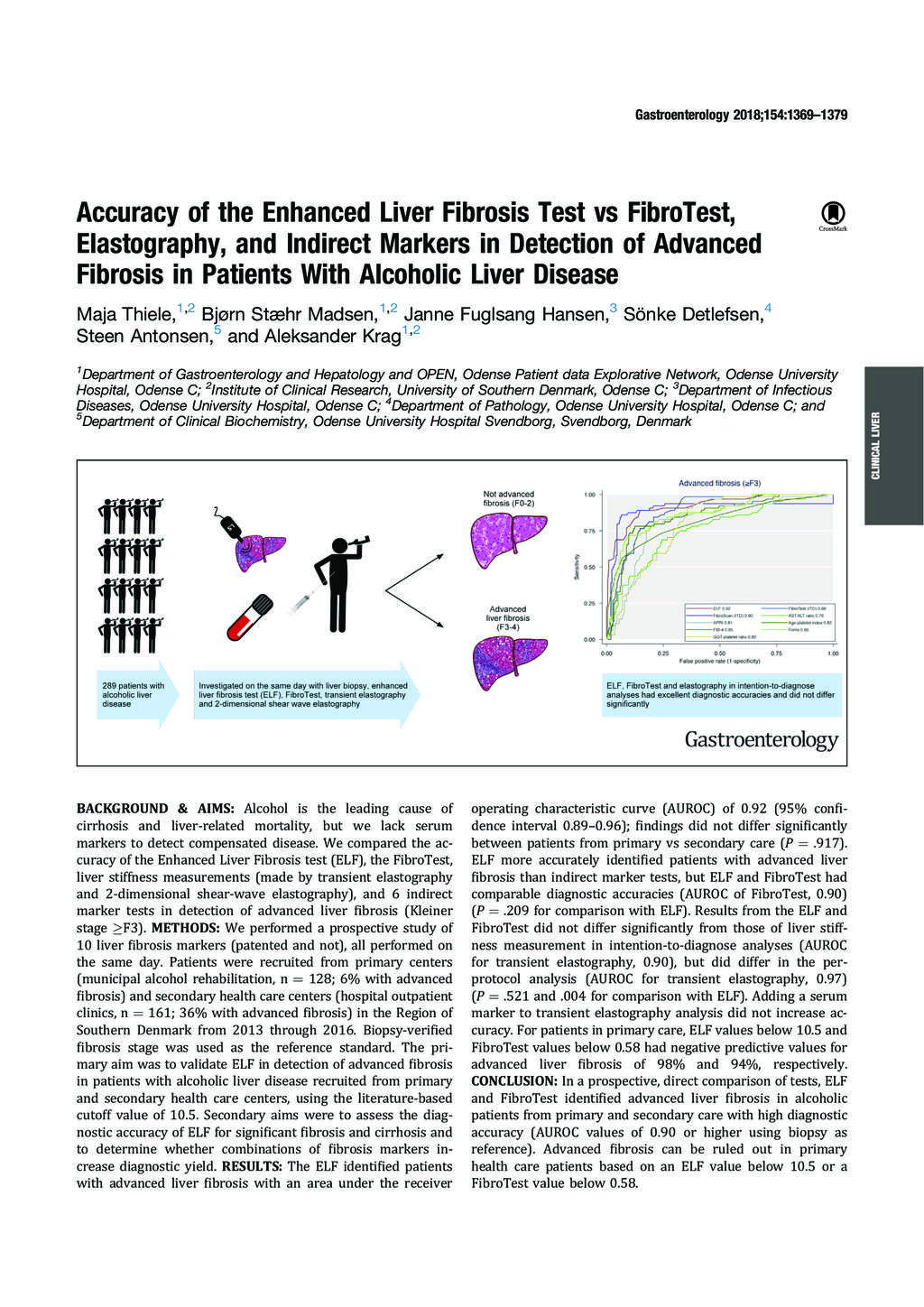
Alcohol is the leading cause of cirrhosis and liver-related mortality, but we lack serum markers to detect compensated disease. We compared the accuracy of the Enhanced Liver Fibrosis test (ELF), the FibroTest, liver stiffness measurements (made by transient elastography and 2-dimensional shear-wave elastography), and 6 indirect marker tests in detection of advanced liver fibrosis (Kleiner stage ≥F3).
METHODS
We performed a prospective study of 10 liver fibrosis markers (patented and not), all performed on the same day. Patients were recruited from primary centers (municipal alcohol rehabilitation, n = 128; 6% with advanced fibrosis) and secondary health care centers (hospital outpatient clinics, n = 161; 36% with advanced fibrosis) in the Region of Southern Denmark from 2013 through 2016. Biopsy-verified fibrosis stage was used as the reference standard. The primary aim was to validate ELF in detection of advanced fibrosis in patients with alcoholic liver disease recruited from primary and secondary health care centers, using the literature-based cutoff value of 10.5. Secondary aims were to assess the diagnostic accuracy of ELF for significant fibrosis and cirrhosis and to determine whether combinations of fibrosis markers increase diagnostic yield.
RESULTS
The ELF identified patients with advanced liver fibrosis with an area under the receiver operating characteristic curve (AUROC) of 0.92 (95% confidence interval 0.89-0.96); findings did not differ significantly between patients from primary vs secondary care (P = .917). ELF more accurately identified patients with advanced liver fibrosis than indirect marker tests, but ELF and FibroTest had comparable diagnostic accuracies (AUROC of FibroTest, 0.90) (P = .209 for comparison with ELF). Results from the ELF and FibroTest did not differ significantly from those of liver stiffness measurement in intention-to-diagnose analyses (AUROC for transient elastography, 0.90), but did differ in the per-protocol analysis (AUROC for transient elastography, 0.97) (P = .521 and .004 for comparison with ELF). Adding a serum marker to transient elastography analysis did not increase accuracy. For patients in primary care, ELF values below 10.5 and FibroTest values below 0.58 had negative predictive values for advanced liver fibrosis of 98% and 94%, respectively.
CONCLUSION
In a prospective, direct comparison of tests, ELF and FibroTest identified advanced liver fibrosis in alcoholic patients from primary and secondary care with high diagnostic accuracy (AUROC values of 0.90 or higher using biopsy as reference). Advanced fibrosis can be ruled out in primary health care patients based on an ELF value below 10.5 or a FibroTest value below 0.58.
Citation Reference: